Cetirizine
"Buy generic cetirizine 10mg online, allergy testing omaha ne."
By: Amy Garlin MD
- Associate Clinical Professor

https://publichealth.berkeley.edu/people/amy-garlin/
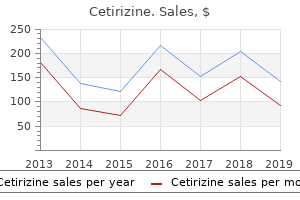
The student is invited to experiment with the various regression options in Excel allergy shots hives cetirizine 5 mg without a prescription. Using Excel for Mac 2008 the steps for finding the line of best fit using Excel for Mac 2008 are given below allergy symptoms loss of voice buy 10mg cetirizine overnight delivery. Step 2: Under the Charts option (tertiary toolbar), we select X Y (Scatter), then click on the first choice. Step 3: To add a trendline, we click on one of the points on the scatterplot to "activate" them (they will appear as X shapes). Step 4: We go to the Chart option on the primary toolbar, and select Add Trendline from the drop-down menu. Step 5: We check the boxes next to Display equation on chart and Display R-squared value on chart. Other types of regression can be viewed by clicking on Type in the Format Trendline window. Use Excel to find a quadratic function (polynomial of power 2) that best fits the data in Exercise 2. You can obtain MathPrint and install it by following the instructions given below. Press [with the cursor next to any item you wish to archive (it will be marked with an asterisk). Method 2: Transfering the MathPrint Operating System from Another Graphing Calculator Press F and Mem and then [on the sending calculator and check that the latest version of the operating system (2. Evaluating logs with bases other than 10 or e cannot be done on a graphing calculator if the MathPrint operating system is not installed. The &Editor MathPrint features can be accessed from the & editor as well as from the home screen. The following table shows examples that illustrate differences between MathPrint in the & editor and Classic mode. Because of the symmetry of the curve, area under the curve between z = 0 and a negative value of z are found in a similar manner. Yes 5 17 A indicates that the exercise asks for a written interpretation or explanation; answers will vary. Domain = 5x x is a real number and x Z 06; range = 5x x is a real number and x Z 06 4. The line will slant up from left to right, will intersect the y-axis at 10, 12, and will be steeper than y = 10x + 1. The line will slant up from left to right, will pass through the origin, and 2 will be less steep than y = x. The line will slant down 31 from left to right, will pass through the origin, and will be steeper than y = - 10x 4. The line will slant down from left to right, will intersect the y-axis at 10, - 12, and will be less steep than 5 y = - 32 x - 1. The graph of y2 is a shift 3 units up of the graph of y1, and y2 has y-intercept 10, 32. The graph of y3 is a shift 4 units down of the graph of y1, and y3 has y-intercept 10, - 42. The graph of y = x - 5 is a shift 5 units down of the graph of y = x, and y = x - 5 has y-intercept 10, - 52. For any x-value, the y2-value is 3 more than the y1-value and the y3-value is 4 less than the y1-value. Approximately (14, 266) y 5 4 x2 + 5x + 6 3 f(x) = 2 x+3 1 -7 -6 -5 -4 -3 -2 -1 -1 -2 -3 -4 -5 1 2 3 x 35. The data are increasing, but these prices seem lower than the trend of the curve indicates.
Therefore allergy shots nyc purchase 5mg cetirizine otc, it is important that clinicians screen records and administer required immunizations at all types of visits allergy shots vs acupuncture cheap cetirizine 10 mg with mastercard, and administer all needed vaccinations simultaneously. Additionally, clinicians should operate reminder/recall systems, in which parents of underimmunized children are prompted by mail or telephone to visit the clinic for immunization. The assessment of clinic-wide immunization levels and feedback of these data to providers have also been shown to increase immunization rates. Immunization schedules and other details of specific vaccines are presented in Chapter 9. Task Force on Community Preventive Services: Recommendations regarding interventions to improve vaccination coverage in children, adolescents, and adults. This may be particularly true with older school-aged children or adolescents who may be seen more rarely for routine health maintenance visits. If the infant develops a problem during the newborn period, a provider who has already met the family is in a better position to maintain rapport and communication with the new parents. In addition to helping establish a relationship between parents and pediatric providers, the prenatal visit can be used to gather information about the parents and the pregnancy, provide information and advice, and identify highrisk situations. A range of information can be provided to parents regarding feeding choices and the benefits of breast feeding; injury prevention, including sleeping position and the appropriate use of car seats; and techniques for managing colic. Potential high-risk situations that may be identified include mental health issues in the parents, a history of domestic violence, or maternal medical problems that may affect the infant. Attention should be directed toward those parts of the body that are most vulnerable to the stresses of sports. The history and physical examination should focus on the following systems: cardiovascular (stenotic lesions, hypertension, surgery), respiratory (asthma), vision, genitourinary (absence or loss of function of one testicle), gastrointestinal (hepatosplenomegaly, hernia), skin (infection), musculoskeletal (inflammation, dysfunction), and neurologic (concussions, uncontrolled seizures). The sports physical should include counseling about medication usage, protective equipment, proper supervision and instruction, injury management, and the emotional aspects of competition and teamwork. For example, protective eyewear, mouth guards, padded goalposts, and efforts to minimize heading the ball should be discussed with a soccer player and his or her parent. The potential for mild menstrual irregularities should be explained to the adolescent female athlete. The pediatric clinician should document the events related to the presenting problem and carefully describe them in the medical record. Treatments and follow-up instructions must be recorded, including when to return to the office if the problem is not ameliorated. Anticipatory guidance should address nutritional needs to maintain growth, cessation of activity when pain occurs, and fluid and electrolyte availability to avoid dehydration. Forty-five minutes is usually enough time for the therapeutic process to evolve, and this time should be protected from interruption. The young child is usually interviewed with the parent; school-aged children and adolescents benefit from time alone with the physician. The pediatrician should know the warning signs of childhood depression and bipolar disorder and have a low threshold for referral of these concerns to the appropriate mental health professional. Twenty-five percent of children and 35% of adolescents have illnesses that meet the definition of a chronic illness. The most common chronic illnesses in pediatric practice include asthma, otitis media with effusion, skin disorders, attention-deficit/hyperactivity disorder, and allergic diseases. The goal of chronic disease management is to optimize quality of life while minimizing the side effects of treatment interventions. Pediatric subspecialty referrals need to be arranged and monitored and results recorded in the chart in an organized manner. Chronic problems often mean chronic use of medications and the need to monitor their use. Documentation should be made in the medical record whenever a prescription is refilled. Finally, an insurance company representative may want a second opinion before authorizing a set of services.
Patients have a positive cross-arm test allergy shots horses discount cetirizine 10mg otc, in which pain is localized to the acromioclavicular joint allergy symptoms coughing itchy throat cheap cetirizine 5 mg online. Radiographs are helpful to assess the degree of injury and to evaluate for a coexisting fracture. Treatment is supportive, with rest and immobilization in a sling followed by progressive rehabilitation. Follow-up treatment for a glenohumeral dislocation in young athletes is controversial. Because of the high risk of recurrence, options for treatment should be individualized, with consideration given to both nonoperative and surgical management. Rotator cuff injuries are common in sports requiring require repetitive overhead motions. Muscle imbalances and injury can cause the position of the humeral head to be abnormal, which may cause impingement of the supraspinatus tendon under the acromial arch. Patients with nontraumatic shoulder instability due to ligamentous and capsular laxity (also known as multidirectional instability) are prone to overuse rotator cuff injury. The athlete presents with a chronic history of pain in the anterior and lateral shoulder, which is increased with overhead activities. Diagnostic workup includes plain radiographs and an outlet view to look for anatomic variability. The rehabilitation of this injury is geared toward reduction of inflammation, improved flexibility, core stabilization, and strengthening of the scapular stabilizers and rotator cuff muscles. A biomechanics evaluation can assist athletes in the recovery process by building sport-specific skills and eliminating substitution patterns. Fracture of the Humerus Fractures of the humerus occur from a severe blow or fall on the shoulder. Careful assessment of the brachial plexus and radial nerves are needed to rule out associated nerve damage. Reduced range of motion of the shoulder Acute traumatic anterior shoulder instability occurs from a significant force applied to the abducted and externally rotated shoulder. Children should be properly conditioned and coached in correct throwing biomechanics. Little League limits 10- to 12-year-old children to 6 innings per week and 13- to 15-year-old children to 9 innings per week. The patient presents with activity-related pain in the lateral aspect of the proximal humerus. Radiographs show widening, sclerosis, and irregularity of the proximal humeral physis. Return to play can only be accomplished after a period of rest has significantly decreased the pain and the athlete has proceeded through a progressive throwing program. Panner Disease Panner disease refers to variations in the normal ossification of the capitellum. The child may have dull aching in the lateral elbow that generally worsens when throwing. Radiographs show an abnormal capitellum, with fragmentation and areas of sclerosis. The natural history of this condition is one of complete resolution of symptoms and ultimately normal ossification of the capitellum.
Over the next few hours allergy forecast for san antonio cetirizine 5mg free shipping, hypoxemia increases and respiratory distress becomes clinically apparent allergy symptoms to shellfish buy 10mg cetirizine with visa, with cyanosis, tachycardia, irritability, and dyspnea. Radiographic evidence of early parenchymal change is the appearance of "fluffy" alveolar infiltrates initially appearing in dependent lung fields, indicative of pulmonary edema. Protein in the air spaces inactivates surfactant, which, combined with damage to type 2 alveolar pneumocytes, leads to a marked deficiency in surfactant content in the lung. As a result, the lung is particularly prone to collapse and to shearing injuries due to the high surface tension required to open collapsed alveoli. Those patients who still show evidence of functional alveolar liquid clearance mechanisms during the first day of their illness have a much higher survival rate than those with evidence of severe epithelial impairment. Pulmonary hypertension, decrease in lung compliance, and increase in airway resistance are also commonly noted. Pathophysiologic changes of modern acute respiratory distress syndrome (low-pressure pulmonary edema). Symptoms Phase 1 (early changes) Normal radiograph Dyspnea, tachypnea, normal chest examination Mild pulmonary hypertension, normoxemic or mild hypoxemia, hypercapnia. Pulmonary hypertension, normal wedge pressure, increased lung permeability, increased lung water, increasing shunt, progressive decrease in compliance, moderate to severe hypoxemia. Progression of abnormalities, increasing shunt fraction, further decrease in compliance, increased minute ventilation, impaired oxygen extraction of hemoglobin. Recurrent pneumonia, progressive lung restriction, impaired tissue oxygenation, impaired oxygen extraction. The mortality rate is greater than 80% at this stage, since resolution is more difficult. This approach has been termed the open-lung strategy and has been the subject of intense scrutiny in recent years (see below). This results in decreased lung volumes and signs of consolidation that are noted clinically and radiographically. Worsening of the hypoxemia with an increasing shunt fraction, as well as a further decrease in lung compliance, are noted. Some patients develop an accelerated fibrosing alveolitis in which fibroblasts and collagen formation in the interstitium are markedly increased. Current investigation centers on the role of growth and differentiation factors, such as transforming growth factor- and platelet-derived growth factor released by resident and nonresident lung cells such as alveolar macrophages, mast cells, neutrophils, alveolar type 2 cells, and fibroblasts. During this phase of the illness, oxygenation defects generally improve, and the lung becomes more fragile and susceptible to barotrauma. Air leak is common among patients still ventilated with high levels of airway pressure at this late stage in their illness. Also, patients have increased amounts of dead space, and difficulties with ventilation are common. Airway compliance remains low, perhaps because of ongoing pulmonary fibrosis and insufficient surfactant production. The mechanisms responsible for increased host susceptibility to infection during this phase are not well understood. However, recent work from a large multicenter trial sponsored by the National Institutes of Health suggests that the tidal volumes used may be important. Those patients ventilated with the lower tidal volume demonstrated fewer extrapulmonary organ failures and an overall 25% decrease in mortality. Death is usually caused by multiorgan failure and systemic hemodynamic instability rather than by hypoxemia. For patients with severe disease or concurrent cardiac dysfunction, consideration can be given to pulmonary artery catheterization to help with fluid management and to allow assessment of mixed venous blood saturation as an index of overall tissue oxygenation. Since secondary infections are common and increase mortality rates strikingly, surveillance for infection is important, requiring appropriate cultures and following the temperature curve and white blood cell count.
Purchase cetirizine 5 mg on-line. Allergy proof your home this spring.
References:
- https://www.hrsa.gov/sites/default/files/publichealth/guidelines/BehavioralHealth/behavioralhealthcareaccess.pdf
- https://www.downeastobgyn.com/wp-content/uploads/2019/09/fact-sheet-vaginal-yeast-infections.pdf
- https://designsinlife.com/wp-content/uploads/2018/12/ltc-product-and-underwriting-guide-12_17_18.pdf
- http://www.faithinradcliff.org/home/140002120/140007394/docs/Plague%20Lessons%20Master.pdf
- https://www.paho.org/gut/dmdocuments/Guia%20para%20el%20manejo%20integral%20del%20recien%20nacido%20grave.pdf